
Abstract
The U.S. long-term care ecosystem remains critical to millions of older adults, people with disabilities, families, and direct care workers. Yet a long-standing, deeply entrenched “caregiving divide” prevents this ecosystem from genuinely delivering what people need to provide and receive long-term care. The caregiving divide operates across six dimensions: ideas, systems, place, resources, power, and narrative. This article describes how this divide shapes and hinders long-term care, with special attention to direct care workers, who form its paid backbone. It also examines its ripple effects among communities and proposes a way forward to reimagine long-term care in this country.
Key Words
long-term care, caregiving, aging, disability, care work, direct care workers, Medicaid, care economy
I became interested in the long-term care ecosystem in 2010, when I discovered a press release announcing a federal grant to establish a historic national resource center for LGBTQ older adults. Research had steadily documented the numerous barriers facing this population, often rooted in a long history of discrimination, and the resource center aimed to address those challenges.
Almost daily, I had been thinking about my older parents thousands of miles away, and wondering what my sister and I would do when the time came to begin accessing professional support. I knew little about this field, so I dove in by taking on a national advocacy role at SAGE, which had received the grant.
Over the years, I have lived through a range of professional and personal experiences, which have shaped what I know about the critical yet beleaguered long-term care ecosystem that supports about 17.6 million older adults and people with disabilities, employs roughly 5.4 million direct care workers, enfolds an estimated 63 million family caregivers, and costs approximately $257 billion in public spending (AARP & National Alliance for Caregiving, 2025; Centers for Medicare & Medicaid Services [CMS], 2023; PHI, n.d.).
In 2015, I began overseeing the advocacy and research division on the direct care workforce at PHI, and serving on various national advisory roles across aging, workforce, and caregiving issues. A year later, in 2016, I barely survived a heart attack that has deepened my understanding of long-term care, along with what I know about being gay, disabled, and Latino. Society has been set up in such a way that systems and institutions, not individual effort, largely determine who makes it through this world and who does not. All of this proves true in long-term care and in the aging process.
Through all these experiences, I have distilled that at the core of long-term care exists a “caregiving divide” shaped by foundational structures, a range of experiences among people who navigate these structures, and the broader systems that either repair or reform them. This article explains caregiving divides, describes how they affect all of us, and proposes ways leaders from different sectors can work together to create a fairer, more accessible long-term care ecosystem.
What Is the Caregiving Divide?
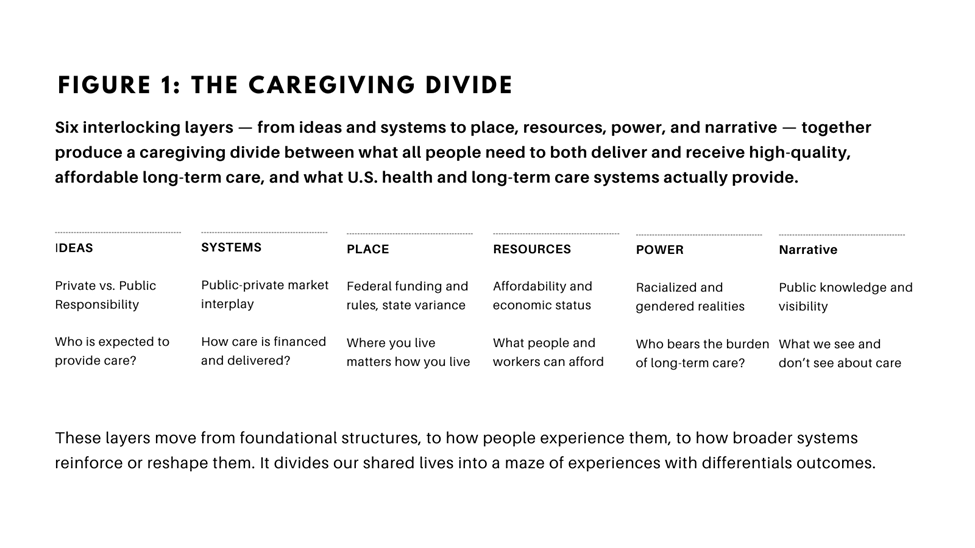
The caregiving divide describes the gap between what people need to deliver and receive long-term care—ongoing assistance with daily living and health-related needs—and what this fractured ecosystem actually provides. This divide operates across six dimensions: ideas (private vs. public responsibility), systems (the public-private market interplay), place (federalism and state-to-state variance), resources (affordability and economic status), power (racialized and gendered realities), and narrative (public knowledge and visibility). See Figure 1, below.
To illustrate how the caregiving divide functions, this article focuses on the direct care workforce, an essential yet undervalued job sector that supports millions of older adults and people with disabilities across long-term care settings.
Ideas. At the core of the caregiving divide is the public debate over long-term care as a social contract: To what extent should responsibility for long-term care delivery rest with families, function as a market service, or be a collective public responsibility?
First, when long-term care is framed as a family duty, policy proposals tend to emphasize personal choice, retirement planning, and means-tested approaches, such as Medicaid. This perspective feeds the mentality behind Medicaid work requirements and other measures that reduce eligibility, while simultaneously limiting the scope of social insurance programs that more closely align with the idea of care as a public good (Congressional Research Service [CRS], 2023). In contrast, under a market-based approach, private insurers, employers, industry associations, and others necessarily understand long-term care as a business proposition that can promote efficiency and even profit, often at the expense of access (KFF, 2024).
Direct care workers illustrate how these competing ideas operate. Their jobs are largely financed by Medicaid, and many of them rely upon Medicaid for their own care, yet policies that defund Medicaid wrongly assume the program is rife with fraud and that healthcare is better left to individual choice and the free market (Carpenter et al., 2023; PHI, n.d). Families who need direct care often cannot afford an agency-based worker and instead turn to the gray market to create workable arrangements—or they forgo care altogether (Genworth Financial, 2024; KFF, 2024).
The caregiving ecosystem is governed by a mix of federal and state regulations and financing mechanisms.
Workers, in turn, navigate these arrangements and continually experience poor-quality jobs because of an under-resourced Medicaid system and limited job-quality requirements for employers. Workers cannot improve their jobs alone; the market relies on their low-wage labor, and Medicaid has reached a breaking point without an alternative financing mechanism in sight (PHI, 2021).
Systems. The caregiving divide operates as a systems problem rooted in the uneasy interplay between public financing and private markets. Long-term services and supports (LTSS; or “long-term care”) are primarily financed through Medicaid, a federal–state entitlement program (Carpenter et al., 2023; KFF, 2024). Yet care delivery itself is largely carried out by private providers, nonprofit organizations, and for-profit firms operating within market constraints.
Families who do not qualify for Medicaid—or who cannot find available providers at Medicaid rates—must rely upon private long-term care insurance, personal savings, or unpaid family care, often at substantial financial strain (KFF, 2024). The result is a fragmented system in which access, quality, and affordability depend heavily upon geography, income, and administrative design rather than on need.
This same divide is evident in the direct care workforce. Direct care workers—numbering roughly 5.4 million nationwide—are employed largely by private homecare agencies, nursing facilities, and consumer-directed arrangements, yet their jobs are predominantly financed by Medicaid reimbursement (Carpenter et al., 2023; PHI, n.d.). When states set inadequate reimbursement rates to contain public spending, many private employers operate on thin margins, constraining wages, benefits, and training investments. In this way, the caregiving divide is not simply about individuals; it reflects a structural misalignment between public responsibility and private delivery.
Place. The variance in long-term care across states and its relationship with the federal government creates another divide. This ecosystem is governed by a mix of federal and state regulations and financing mechanisms (CRS, 2024; KFF, 2024). Where a person lives determines what services are available and affordable, creating stark divides across state lines and regions. Also, while states can design policies that address their unique realities and advance the field, these innovations rarely scale successfully to reach other parts of the country.
In terms of the direct care workforce, a state can be assessed based on its worker-friendly policies and on how workers fare economically. In essence, data shows a divided country: Generally, direct care workers in states that have better jobs and financial security, and workers in the rest of the country (PHI, 2024). Also, because direct care worker training requirements vary by state, setting, and occupation, workers lack the option to transfer their training from one job to the next (PHI, 2021). During the early stages of the COVID-19 pandemic, this patchwork approach became evident. As New York City emerged as the epicenter of COVID and direct care workers were desperately needed, trained direct care workers from nearby states could not drive to the city to offer support (PHI, 2020).
Resources. In many ways, a person’s access to long-term care depends upon their ability to afford it, a challenge exacerbated by the exorbitant costs of home care, assisted living, and nursing homes (Genworth Financial, 2024). Because Medicaid only supports low-income individuals, millions of middle-income people are left with few options (Pearson et al., 2019). They often cannot afford long-term care on their own, and because they do not qualify for Medicaid, they must either go without professional care or spend down their assets and savings to become eligible.
Higher-income people also have stronger retirement planning options, savings histories, and access to health and social support systems that can ease the challenges during this moment (Finkelstein et al., 2022). The market and policy failure dynamics here are especially salient: Private long-term care insurance policies are fledgling, healthcare and long-term care costs will only rise in the years ahead, and insufficient public financing leaves workers and families bearing costs that a national social insurance approach to long-term care could help resolve.
‘By treating long-term care as a private matter rather than essential infrastructure, the caregiving divide traps direct-care workers in poverty.’
In direct care, too many workers cannot afford to take or remain in these low-wage roles and are often pulled away by modestly better-paying job sectors such as fast food and retail. For workers, this results in entrenched poverty with limited advancement paths, and for families who need care, this means vacant roles, disrupted care continuity, and compromised care. Low-wage jobs also increase public benefit access and reduce consumer spending. Improperly trained or supported workers can lead to costly accidents and preventable emergency department readmissions, which ultimately cost the public what it could have avoided had it simply invested early on in a well-resourced long-term care system. What policymakers and industry leaders believe is saving costs today will be extremely expensive tomorrow, dividing even further those who can afford care from those who cannot.
Power. In a deeply racialized economy, long-term care access and outcomes are shaped by racialized and gendered dimensions. Families with greater wealth and social capital—disproportionately white—can more readily secure home care, while Black and Latino people are more likely to be prematurely institutionalized in often low-quality nursing homes, a trend that reared its deathly head during the COVID-19 crisis (Centers for Disease Control and Prevention [CDC], 2022; Sloane et al., 2021).
As a national policy professional who has worked at the intersection of aging, long-term care, and the workforce, over the years I’ve seen that many national organizations in those areas rarely propose more than a few race-explicit policy solutions to improve care, even though such ideas would benefit everyone. Consider a policy to establish multilingual training and education for immigrant direct-care workers that would boost their skills and economic mobility while expanding workforce capacity in already-stretched areas for everyone. The current muting of such approaches will amplify these problems for all of us in the years ahead and will require a return to such thinking.
Women—especially Black, Latina, and immigrant women—often bear the responsibilities of family caregiving and disproportionately comprise the direct care workforce, reflecting how gender norms assign women care roles while devaluing their skilled work (Center for American Progress, 2023). From the decades-long exclusion of domestic workers during the New Deal in the 1930s, led largely by a Southern delegation hyped into preserving the post-slavery, Jim Crow era, to decades of Medicaid decisions rooted in racist ideals, the effect has been a profoundly different and punishing reality for people of color as long-term care recipients and direct care workers (Gillin, 2019; Nolen et al., 2020).
Complicating this picture is the fact that as people live longer and the country ages, so does its workforce. Already, about one in four direct care workers is ages 55 and older (PHI, 2025). However, this sector will need to do what other industries have failed to accomplish: reduce the ageism that is so pronounced in the workplaceviahiring discrimination, forced retirement expectations, limited training opportunities, and subtle cultural signals that older workers are “past their prime” (AARP, 2023).
Narrative. As a Leadership and Society Fellow at the University of Chicago, I recently completed a structured qualitative analysis of news articles on caregiving and long-term care, examining framing, system visibility, sourcing, governance, and other relevant factors (Espinoza, 2026). The study found that most coverage examines only partial aspects of the caregiving system rather than the system as an integrated whole. Many articles identified problems with long-term care but did not name their sources nor offer solutions. And while financing and Medicaid are referenced in many of these news articles, they are rarely explained in depth.
‘Philanthropy can catalyze change by funding both immediate needs and long-term care system transformation.’
This study mirrors my experience. In 2015, when I began working on direct care workforce issues, most news stories about home-care workers were either sensationalized accounts of workers who had stolen from their clients’ homes—the “home care thief” trope—or occasional stories about wage needs in direct care.
All these patterns dampen policy imagination and constrain public understanding, as evidenced by recent research showing that people often confuse care as healthcare and consider care at home to be less skilled and less important. They also perceive home-care delivery as a personal characteristic rather than a set of skills and an occupation that merits professional status (FrameWorks Institute, 2023).
The Ripple Effects of a Fragmented Ecosystem
These six interlocking layers produce a set of cascading harms for individuals and families, direct care workers, employers, and the broader economy.
Individuals and Families. The caregiving divide leaves families to shoulder risks that should be shared collectively, forcing painful tradeoffs between work, income, and care. Fragmented systems, uneven state policies, and unaffordable costs push many families—especially from communities of color—to seek lower-quality or institutional care. Limited public visibility of caregiving solutions keeps these struggles off the policy agenda.
Direct Care Workers. The caregiving divide entrenches a low-wage, precarious labor market for direct care workers, rooted in ideas that devalue care as “natural” rather than skilled work. Fragmented financing and uneven state standards produce unstable jobs, limited career pathways, and high turnover, disproportionately affecting women, immigrants, and workers of color. Because policymaking remains largely reserved for elites, workers have little real voice in shaping the systems that govern their work.
Employers in Long-Term Care. The caregiving divide constrains long-term care employers through misaligned payment systems, chronic underfunding, and highly variable state rules that shape their ability to pay living wages or invest in care quality. These conditions drive persistent workforce shortages, high turnover, and rising training costs. Public misunderstanding and crisis-driven narratives about long-term care further erode trust and make recruitment harder.
The Broader Economy. By treating long-term care as a private matter rather than essential infrastructure, the caregiving divide traps direct-care workers in poverty. Unaffordable long-term care dampens household savings, productivity, consumer spending, and regional economic growth. The racialized and gendered barriers facing direct-care workers also reinforces broader inequities in income and wealth across generations.
A Way Forward on the Caregiving Divide
Individuals and families can close the caregiving divide by treating long-term care not as a private burden but as a collective concern that merits their voices. By sharing their experiences and advocating for better institutional supports in their communities, families can challenge the idea that long-term care should be endured in isolation. They can also support direct-care workers’ rights, push employers and policymakers for affordable options, and help shift public narratives so care is seen as essential social infrastructure rather than a personal misfortune, or as a skilled job versus a personality trait.
Social change organizations can improve the long-term care ecosystem by advancing structural reforms across markets, states, and federal policy. They can build broad coalitions that link family caregivers, direct care workers, and people receiving care with all relevant institutional actors. They could advance policy campaigns that reform this ecosystem, as well as develop narratives that make long-term care and its workforce more visible with solutions articulated at the systemic level.
Government leaders can redefine long-term care as a public responsibility and invest accordingly. This means aligning federal and state financing with competitive direct-care wages and high-quality long-term services and supports, strong labor standards, and universal access to long-term care. It also means reducing geographic inequities, among other divides, and making long-term care benefits and direct-care worker training and credentials portable across states.
Businesses of all types and sizes can act by recognizing that long-term care is a widespread need affecting their employees and central to their bottom lines. They can provide paid family leave, flexible schedules, and family caregiver benefits, while providing proper compensation, training, and career pathways. Larger firms, in particular, can use their purchasing power and policy voice as industry advocates to call for stronger public investment in long-term care.
Other industry actors, such as unions, workforce-development entities, tech innovators, and private payors, can help redesign systems so they work better for families and workers alike. Providers can invest in worker training, career pathways, and participatory management. Unions can continue to organize to raise standards and bargaining power while establishing even more state models for labor-management approaches to job quality in direct care. Training institutions can enhance their curricula to ensure they reflect current core and specialized competencies and their methodologies to reach adult learners. And technology firms can build evidence-based, worker/consumer-informed tools that reduce administrative burden, strengthen jobs, and improve long-term care delivery.
Philanthropy can catalyze change by funding both immediate needs and long-term care system transformation. This includes investing in innovative models of home- and community-based care, efforts to improve job quality and support worker organizing, research that clarifies gaps, and research-informed narrative strategies that elevate long-term care solutions in the public imagination.
Impact investors can align capital with long-term care by backing business models that prioritize quality jobs, affordability, and equitable access. They can support mission-driven providers, workforce development initiatives, and technologies that improve care coordination and direct care jobs, while insisting on measurable social outcomes alongside financial returns.
Designing the Future of Care
After 15 years of leading social change initiatives in the nonprofit sector, I pivoted last fall to reflect upon my next career chapter by joining the Leadership & Society Fellows program at the University of Chicago. Reimagining our broken long-term care ecosystem will require a range of public-private solutions, and social enterprise in particular has the potential to build upon what’s working in this system. It can scale what’s effective and step in where others have failed.
This past April, I launched The CareWorks Project, an innovation lab and consulting studio to help leaders transform how the long-term care ecosystem system functions. We aim to ensure that people can live with dignity, workers can thrive, and communities can rely on care that truly works.
We’re working with leaders from all walks of life to realize a deeply held, shared belief: A future that honors the people who give and receive care is within reach—but we will need to close the caregiving divide together to fully grasp it.
Robert Espinoza, MPA, is founder and CEO of The CareWorks Project, Asbury Park, NJ, and Leadership & Society Fellow at the University of Chicago. He may be reached at robert@careworksproject.com.
Photo credit: Shutterstock/Juan Aizpuru
References
AARP. (2023). The value of experience: Age discrimination against older workers persists. https://www.aarp.org/work/working-at-50-plus/info-2023/age-discrimination-research.html
AARP & National Alliance for Caregiving. (2025, July 24). Caregiving in the U.S. 2025 [Report]. https://www.aarp.org/pri/topics/ltss/family-caregiving/caregiving-in-the-us-2025/
Center for American Progress. (2023). Direct care worker pay and benefits are low despite high demand for services. https://www.americanprogress.org/article/direct-care-worker-pay-and-benefits-are-low-despite-high-demand-for-services/
Centers for Disease Control and Prevention. (2022). COVID-19 in nursing homes. U.S. Department of Health and Human Services. https://www.cdc.gov/coronavirus/2019-ncov/hcp/long-term-care.html
Carpenter, A., Stepanczuk, C., & Wysocki, A. (2023). Medicaid long-term services and supports (LTSS) user characteristics: Results from the CMS LTSS user characteristics survey. U.S. Department for Health and Human Services, Centers for Medicare and Medicaid Services. https://www.medicaid.gov/medicaid/long-term-services-supports/downloads/ltss-user-character-brief-2023.pdf
Congressional Research Service. (2023). Medicaid work requirements: Background and current status (IF11168). https://crsreports.congress.gov/product/pdf/IF/IF11168
Congressional Research Service. (2024). Medicaid: An overview (R43357). https://crsreports.congress.gov/product/pdf/R/R43357
Espinoza, R. (2026). Designing a caregiving-focused news outlet: Journalism, public knowledge, and accountability in the caregiving economy [Unpublished manuscript].
Finkelstein, D. M., Harding, J. F., Paulsell, D., English, B., Hijjawi, G. R., & Ng’andu, J. (2022). Economic well-being and health: The role of income support programs in promoting health and advancing health equity. Health Affairs. https://www.healthaffairs.org/doi/10.1377/hlthaff.2022.00846
FrameWorks Institute. (2023). Framing care work: How the public understands care and what that means for change. https://www.frameworksinstitute.org/publication/framing-care-work/
Genworth Financial. (2024). Cost of care survey 2023: Median annual costs of long-term care services. https://www.genworth.com/aging-and-you/finances/cost-of-care.html
Gillin, J. (2019, July 8). How the New Deal left domestic workers behind. VICE. https://www.vice.com/en/article/how-the-new-deal-left-domestic-workers-behind/
KFF. (2024). 10 things to know about Medicaid and long-term services and supports (LTSS). https://www.kff.org/medicaid/issue-brief/10-things-to-know-about-medicaid-and-long-term-services-and-supports/
Nolen, L. T., Beckman, A. L., & Sandoe, E. (2020, September 1). How foundational moments in Medicaid’s history reinforced rather than eliminated racial health disparities. Health Affairs Forefront. https://www.healthaffairs.org/content/forefront/foundational-moments-medicaid-s-history-reinforced-rather-than-eliminated-racial-health
Pearson, C. F., Quinn, C. C., Loganathan, S., Datta, A. R., Mace, B. B., & Grabowski, D. C. (2019). The forgotten middle: Many middle-income seniors will have insufficient resources for housing and health care. Health Affairs, 38(5), 101377. https://doi.org/10.1377/hlthaff.2018.05233
PHI. (n.d.). Understanding the direct care workforce: Key facts. PHI. https://www.phinational.org/policy-research/key-facts-faq/
PHI. (2020). Would you stay? The experiences of direct care workers and their implications for the future of care. PHI. https://www.phinational.org/caringforthefuture/wouldyoustay//
PHI. (2021). Caring for the future: The power and potential of America’s direct care workforce. PHI. https://www.phinational.org/caringforthefuture/
PHI. (2024). The Direct Care Workforce State Index [Interactive tool]. https://www.phinational.org/state-index-tool/
PHI. (2025). Workforce data center. https://www.phinational.org/policy-research/workforce-data-center/.
Sloane, P. D., Yearby, R., Konetzka, R. T., Li, Y., Espinoza, R., & Zimmerman, S. (2021). Addressing systemic racism in nursing homes: A time for action. Journal of the American Medical Directors Association, 22(4), 886–892. https://doi.org/10.1016/j.jamda.2021.02.023











