
A growing number of individuals are choosing to receive their Medicare benefits through Medicare Advantage (MA). In addition to Medicare-covered benefits, MA plans can offer supplemental benefits, like vision and dental coverage, and lower cost-sharing compared to original fee-for-service Medicare. Traditionally, these supplemental benefits have been limited to those that are primarily health-related, but recent congressional action allows MA plans to offer a wider variety of benefits for the chronically ill population through new “Special Supplemental Benefits for the Chronically Ill” (SSBCI).
In addition to complex medical needs, individuals with chronic conditions have a number of functional and social needs, which significantly impact health. SSBCI enable MA plans to address a broader set of member needs and provide more person-centered and holistic care. Although resources for these benefits are limited, recent growth in the number of MA plans offering SSBCI indicates that MA plans recognize the potential of SSBCI to improve care for members with chronic illnesses.
CHRONIC Care Act Implementation
In 2018, Congress passed the Creating High-Quality Results and Outcomes Necessary to Improve Chronic (CHRONIC) Care Act as part of the Bipartisan Budget Act of 2018, creating SSBCI. The introduction of SSBCI marked a significant turning point in Medicare policy as plans were, for the first time, able to offer non-primarily health-related supplemental benefits, including services to address social determinants of health.
Since SSBCI were first made available in Plan Year 2020, the number of plans choosing to offer them has grown substantially.
SSBCI are limited to beneficiaries who meet the three-part criteria outlined in the CHRONIC Care Act: diagnosis of at least one chronic condition; high risk of hospitalization; and requiring intensive care coordination. The CHRONIC Care Act also waived the uniformity requirement for SSBCI, meaning that MA plans do not have to provide equivalent services to all beneficiaries, and can tailor services according to individual need. Following the creation of SSBCI, the Centers for Medicare & Medicaid Services (CMS) released guidance outlining 10, non-exhaustive examples of benefits MA plans can offer as SSBCI.
As SSBCI were realized in legislation, simultaneously, CMS introduced flexibility to allow MA plans to offer new types of primarily health-related supplemental benefits. In their 2018 guidance, CMS expanded the types of supplemental benefits MA plans could offer to allow for benefits such as in-home support services and caregiver supports. While these benefits are not the focus of this piece, coupled with the introduction of SSBCI, legislators and the administration signaled their support for using existing resources to provide services that help to meet social determinants of health and long-term services and support needs in these policies.
SSBCI: A Current Snapshot
Since SSBCI were first made available in Plan Year 2020, the number of plans choosing to offer SSBCI has grown substantially, from 267 plans offering at least one SSBCI in 2020 to 942 plans in 2021—a nearly fourfold increase (see Table 1, below). This marks an increase from 5 percent of plans in 2020 offering at least one SSBCI to 15 percent of plans in 2021. (ATI Advisory analysis of CMS Plan Benefit Package [PBP] files includes employer plans and excludes Prescription Drug Plans, Medicare-Medicaid Plans, Part B-only plans and PACE.)
Table 1: Plans Offering SSBCI
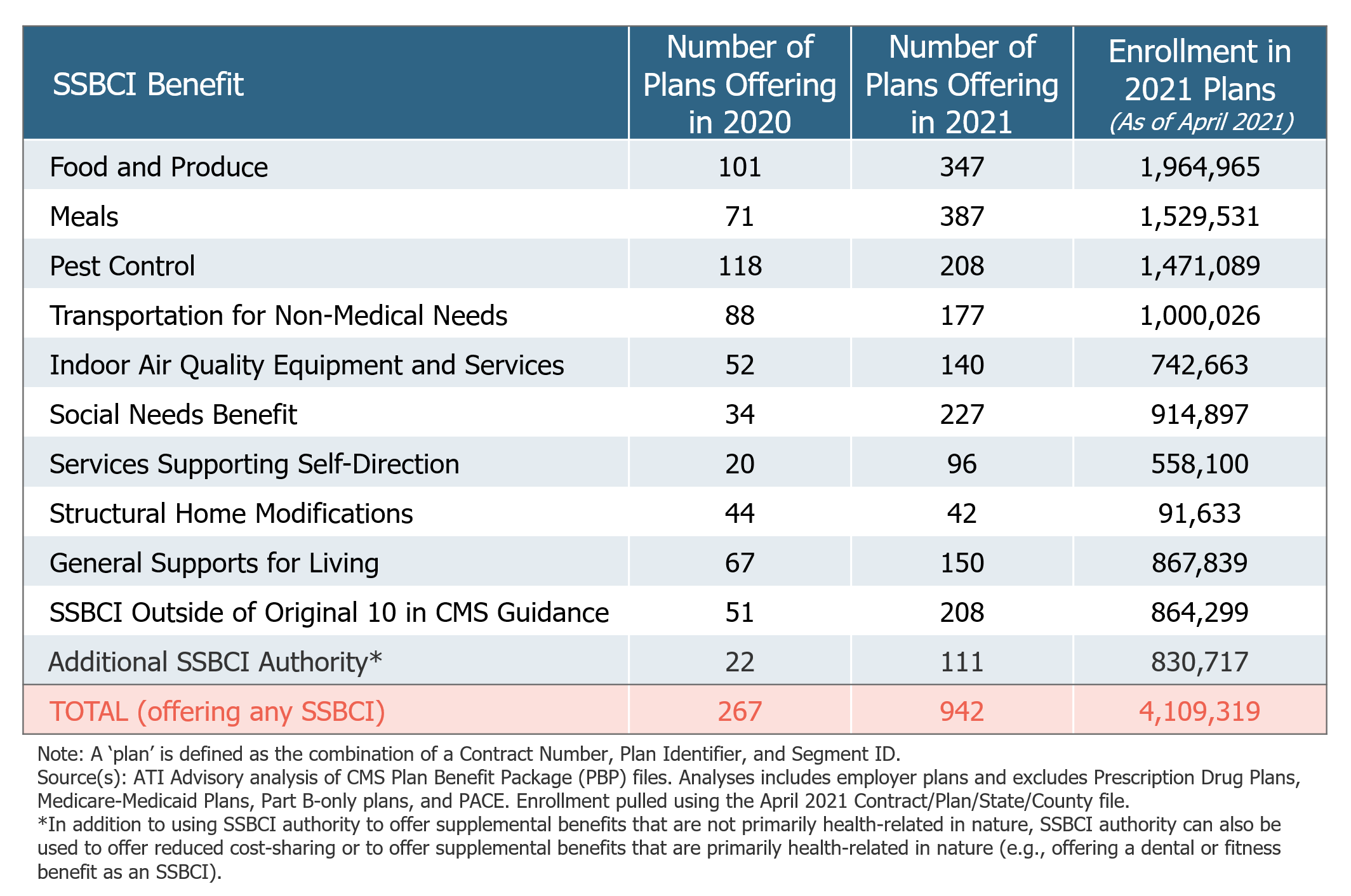
In 2021, the most popular SSBCI include Meals, Food and Produce and Social Needs Benefits. Interviews with health plans highlighted the critical role of food and social isolation services to meet the needs of Medicare beneficiaries during the COVID-19 pandemic and allow beneficiaries to remain safely at home. Additionally, several insurers are offering other SSBCI not outlined in CMS’s original guidance. Examples of these benefits for 2021 include Virtual Visits, Grocery Shopping and Delivery, and Prescription Pickup.
The Potential in Medicare Advantage
The introduction of SSBCI presents a unique opportunity for MA plans to offer a range of new and innovative benefits. This comes at a time when the Medicare population, and with it, the MA population, is growing rapidly. More than 10,000 individuals become eligible for Medicare every day, and as of 2021, MA covers 43 percent of all Medicare-eligible beneficiaries.
The increased number of plans and insurers choosing to offer SSBCI indicates that plans are willing to use this authority to innovate and test benefits to evaluate their potential value, despite an incomplete evidence base. Moreover, the increase in the number of plans choosing to offer services outside of the examples CMS originally outlined signals that MA plans are willing to use this authority to innovate. We expect to see continued growth in these benefits as plans look for ways to compete within an increasingly competitive MA market.
It is vital to recognize the hurdles preventing MA plans from forming partnerships with non-medical providers to deliver these new benefits.
While SSBCI have seen a significant increase, it is vital to recognize the operational and administrative hurdles that prevent MA plans from successfully forming partnerships with non-medical providers to deliver these new benefits. To help maximize the potential of these new benefits, ATI Advisory (ATI) and the Long-Term Quality Alliance (LTQA) released a consensus-based set of Guiding Principles to guide SSBCI implementation, as well as a report outlining strategies for plans and providers to address potential roadblocks.
Although early in their implementation, SSBCI represent an opportunity for MA plans to offer holistic, person-centered care to chronically ill beneficiaries. While plans and providers must collaborate to overcome obstacles standing in the way of offering SSBCI, these partnerships will fundamentally help realize the vision of the CHRONIC Care Act: to better serve Medicare beneficiaries with complex care needs.
Visit our landing page on the ATI Advisory website to learn more about ATI and LTQA’s work on SSBCI and non-medical supplemental benefits in Medicare Advantage, including resources for plans, providers, and policymakers. ATI and LTQA will release a second Roadmap Report and Policy Brief later in 2021 with updated insights.
Elexa Rallos is an Analyst at ATI Advisory in Washington, DC. Claire Jensen is the Policy and Communications Manager for the Long-Term Quality Alliance in Washington, DC.











