
Abstract:
This article examines healthcare-based approaches to reducing social isolation and loneliness among older adults. It reviews a variety of programs in the United States and looks at how they alleviate loneliness, foster connectedness, and improve health among socially isolated elders.
Key Words:
social isolation, loneliness, healthcare, connectedness, Medicare, CareMore, Aspire
“Sara” is 66 years old. For most of her life she was proudly self-sufficient. She raised a son, taught school and earned a master’s degree. Five years ago, as she was working toward a doctorate, Sara was in a car accident that left her dependent upon a walker. She gained weight. She experienced irregular heartbeats and dizzy spells. Her physician diagnosed her with postural orthostatic tachycardia syndrome, a condition that affects blood flow and can cause fainting. Sara’s doctor advised her that it was no longer safe for her to drive. Distant from her friends and uncomfortable with the way she looked, as well as her impaired mobility, Sara stopped socializing. She sank into a deep depression. Things seemed hopeless.
And then Angelica called.
A Hidden Epidemic
Loneliness among older Americans has reached alarming levels. Up to 43 percent of American adults older than age 60 report feeling lonely on a regular basis (Perissinotto, CenzerI, and Covinsky, 2012). Older Americans are particularly susceptible to persistent loneliness because 28 percent of people ages 65 and older, or 13.8 million people, live alone (National Institute on Aging, 2019). But social isolation is not the same as loneliness. The first is a physical state, the second, “the subjective feeling that you’re lacking the social connections you need” (Murthy, 2020). Nevertheless, as the National Institute on Aging reports, “people who find themselves unexpectedly alone due to the death of a spouse or partner, separation from friends or family, retirement, loss of mobility, and lack of transportation are at particular risk” for both social isolation and loneliness (National Institute on Aging, 2019).
Health providers see loneliness as an impediment to good health. Loneliness puts older people at higher risk for high blood pressure, heart disease, obesity, a weakened immune system, anxiety, depression, cognitive decline, Alzheimer’s disease, and even death (National Institute on Aging, 2019). Loneliness can increase a person’s risk of mortality by up to 50 percent, which exceeds mortality risks associated with air pollution, obesity, and excessive alcohol use (Holt-Lunstad, Smith, and Layton, 2010).
This means healthcare systems have an obligation to treat loneliness as what it is—a health problem that affects millions of Americans. Though loneliness has not historically been spoken of in these terms, new research into the condition has led many organizations to begin to address its effects on health outcomes. This article will explore this work and offer a look at some of the more well-known interventions.
The CareMore and Aspire Model
CareMore and Aspire Health comprise an integrated care delivery system that provides care to more than 180,000 high-risk, high-need Medicare and Medicaid patients. A large percentage of the system’s patients are older adults, and many experience multiple comorbidities. Because CareMore and Aspire operate largely under a capitated payment model, its clinicians are not compensated for individual services, but are instead incentivized to achieve positive health outcomes. This means caring for patients in between times of medical care as well as during patient clinical appointments. For example, the system helps people with diabetes learn to prepare and consume more nutritional meals. Its behavioral health specialists help patients struggling with substance use disorders cope with addiction. And its community health workers partner with landlords to find housing insecure patients a place to live, and food banks to ensure patients have food to eat.
In 2017, as an increasing amount of research indicated that loneliness was a substantial impediment to positive health outcomes, CareMore decided that it was the responsibility of providers to address loneliness as they would any other serious determinant of health. The health system appointed a Togetherness Officer, who helped to launch its Togetherness program, the nation’s first-of-its-kind initiative designed specifically to reduce the negative health effects of loneliness among a cohort of patients.
Assessing Risk
Patients are referred to the Togetherness program by an integrated care team (e.g., physicians, nurses, case managers, clinical pharmacists, mental health and substance use disorder specialists), and they can also self-refer. Full time Social Care Partners (SCPs)—community health workers (CHWs) who have backgrounds in social work, counseling, and community resources are responsible for processing patients into the program. SCPs perform psychosocial assessments, screening for barriers to connectedness such as lack of transportation, mobility difficulties, or insecurities regarding attending functions without a partner, which is common among people who have recently lost a spouse. Recently the program has been extended to caregivers of patients, as they also often suffer from loneliness.
Based on this information, SCPs determine whether patients who become members of the Togetherness program are at high-, medium-, or low-risk for loneliness. High-risk members typically have no social support system as well as complex health and psychosocial conditions such as congestive heart failure, cancer, and depression. Often, they contend with legal and family conflicts. At a recent meeting, which is called a “high-risk huddle,” the care team reviewed a cohort of eight high-risk members, six of whom had suicidal ideation. Social care partners remain in close contact with these members, calling at least once a week and designing a personalized care plan intervention to address barriers to socializing. Such interventions are individualized and include connecting members with community resources, mental health and substance use disorder supports and services, and other healthcare services to address their barriers to socialization.
Trained social work interns under the guidance of a licensed clinical social worker also make frequent home visits to this cohort. The goal of such visits is to reduce social isolation and build trust. For example, on one home visit, an intern copied a high-risk member’s phone book in large print because she was having trouble reading her friends’ phone numbers. Later that day, the member taught the intern to play card the game “Hand and Foot.” Both reported that they felt they were helping one another. The member gained a sense of giving back for all the help and companionship the intern had provided.
Patients are referred to the Togetherness program by an integrated care team, and they can self-refer.
On the other end of the spectrum, low-risk members may have some social connections, but they typically spend their days in isolation. They may live with someone—a son or daughter who works all day, for example—but almost all of their time is spent alone. These members generally don’t have complex health conditions, and it is sufficient for SCPs to check in on them once a month.
A ‘Health Outcomes’ Approach
It’s crucial to understand that the CareMore approach to loneliness is deeply rooted in improving health outcomes. Internal research shows that lonely patients are less likely to take their medications or show up for appointments—behaviors that usually result in chronic conditions going untreated and worsening over time.
Knowing this, one of the primary goals of SCPs is to engage in care coordination and help participants adhere to their care plans. They remind patients to attend appointments, refill medications, help connect them to mental health and substance use disorder supports and services, and work with them to obtain durable medical equipment. When a physician recently alerted an SCP that a member was due for a heart exam, the SCP brought it up during her scheduled call and helped the member to schedule the appointment.
Concurrent with the launch of the Togetherness program, the health system began to reconfigure its Care Centers to include social spaces, and introduced classes and other social events. The SCP appears in person at some of these identified Care Centers. The goal was to make healthcare a source of social connectedness. Prior to the COVID-19 outbreak, many Care Centers had become lively places where patients interacted with clinicians and each other. One patient, a blues guitarist, started giving guitar lessons in his neighborhood Care Center.
Also, because they have backgrounds in community health, SCPs refer participants to outside resources where they can socialize with others. Many older adults start attending lunchtime activities at local senior centers. SCPs also help address social drivers of health; for example, connecting food insecure members with food banks and meal delivery programs.
Lastly, CareMore understands the correlation between physical activity and loneliness, so they often refer participants to programs such as Nifty after Fifty, an exercise program for older adults. In addition to promoting exercise through gyms located in Care Centers, Nifty after Fifty also organizes group social activities for participants, including monthly movie matinees and themed potluck parties.
All of these interactions are initiated first and foremost to bolster quality of life and health outcomes that are either rooted in loneliness or adjacent to its most pernicious effects. Those who participate in fitness classes not only get to meet with others at the gym, they also report “significantly better physical and emotional health and lower impairment” (Hamar et al., 2013). Similarly, aerobic exercise has been shown to improve cognitive functioning in older adults (Williams, 2019).
Sara’s Story
Sara was referred to the Togetherness program by the House Call team for isolation and poor social support. Angelica, a Social Care Partner (SCP) based in Southern California, started calling Sara, who lives in Ohio, regularly.
“We talked kind of constantly,” says Sara. “And with every talk Angelica helped me to see my worth. She got me to think about what it would take for me to be happy.”
Though Sara says she and Angelica initially connected over their shared love of dogs, their conversations soon turned toward more serious matters. Angelica sent Sara brochures for local public and nonprofit transportation organizations that would enable her to go to the grocery store and attend classes at her local senior center. (Sara’s transportation to and from medical appointments is paid for by her health plan as part of her healthcare package.)
Embarrassed by her incontinence and unable to wear dentures due to chronic dry mouth, Sara says she was “terrified” to go out in public. But with Angelica’s encouragement, she started attending a local class on chronic pain management. Sara soon signed up for additional classes in stained glass and quilting.
The health system’s experience indicates that when people feel cared about by others, they care a little bit more about themselves. For instance, Angelica sent Sara information about healthful eating and proper nutrition, and encouraged her to go to the local library to find information about the relationship between health and diet. Soon, Sara cut out gluten and incorporated more fruits and vegetables into her diet. “I had my cheerleader out in California and she kept getting prouder and prouder,” Sara says of the inspiration she received from Angelica, virtually. “She sent me cards with inspirational quotes . . . always handwritten, always personal.”
Sara shed 37 pounds in about six months. Sara’s improved health is not an anomaly. CareMore’s initial published outcomes since launching the Togetherness program showed that it was on the right track. The initial results showed a 57 percent increase in exercise program participation among participants and, crucially, a reduction in their hospital admissions.
Phone Pals
At the core of the Togetherness program is the “Phone Pal” program, in which employee volunteers make weekly calls to older participants, trying to match Phone Pals by shared interests. Pals connect with company employees at least once each week on 15- to 30-minute calls during which they chat about a variety of subjects.
In addition to her SCP, Sara also speaks with her Phone Pal, Veronica, a vice president of Operations. Both are quilters and share a love of crafting. Sara says Veronica never misses a call. Given Veronica’s role as a busy healthcare executive, that surprises her. “She makes me the priority. There has to be a reason I have this much value that people are making me feel whole again.”
Measuring Results
Since the launch of Togetherness three years ago, more than 3,700 patients have enrolled in the program. Nearly 600 employee Phone Pals and Social Care Partners have made approximately 130,000 calls to members and more than 7,000 connections to community resources.
A recent study compared the outcomes of 1,000 enrolled Togetherness participants to those of patients who were referred to the program but were not enrolled during the period studied. Based on responses to the three-question UCLA Loneliness Scale and the PHQ-9 Patient Depression Questionnaire, lower rates of depression and loneliness were observed among program participants. The latest data also show 43 percent lower emergency room use, 8 percent lower hospital admissions, and a reduction in Healthcare Effectiveness Data and Information Set gaps for Togetherness participants.
Based on the general profile of Togetherness participants, who largely require higher engagement in other CareMore and Aspire programs, the observed clinical and non-clinical effects are a testament to the totality of the integrated health system’s model on these patients, prompted by the Togetherness program.
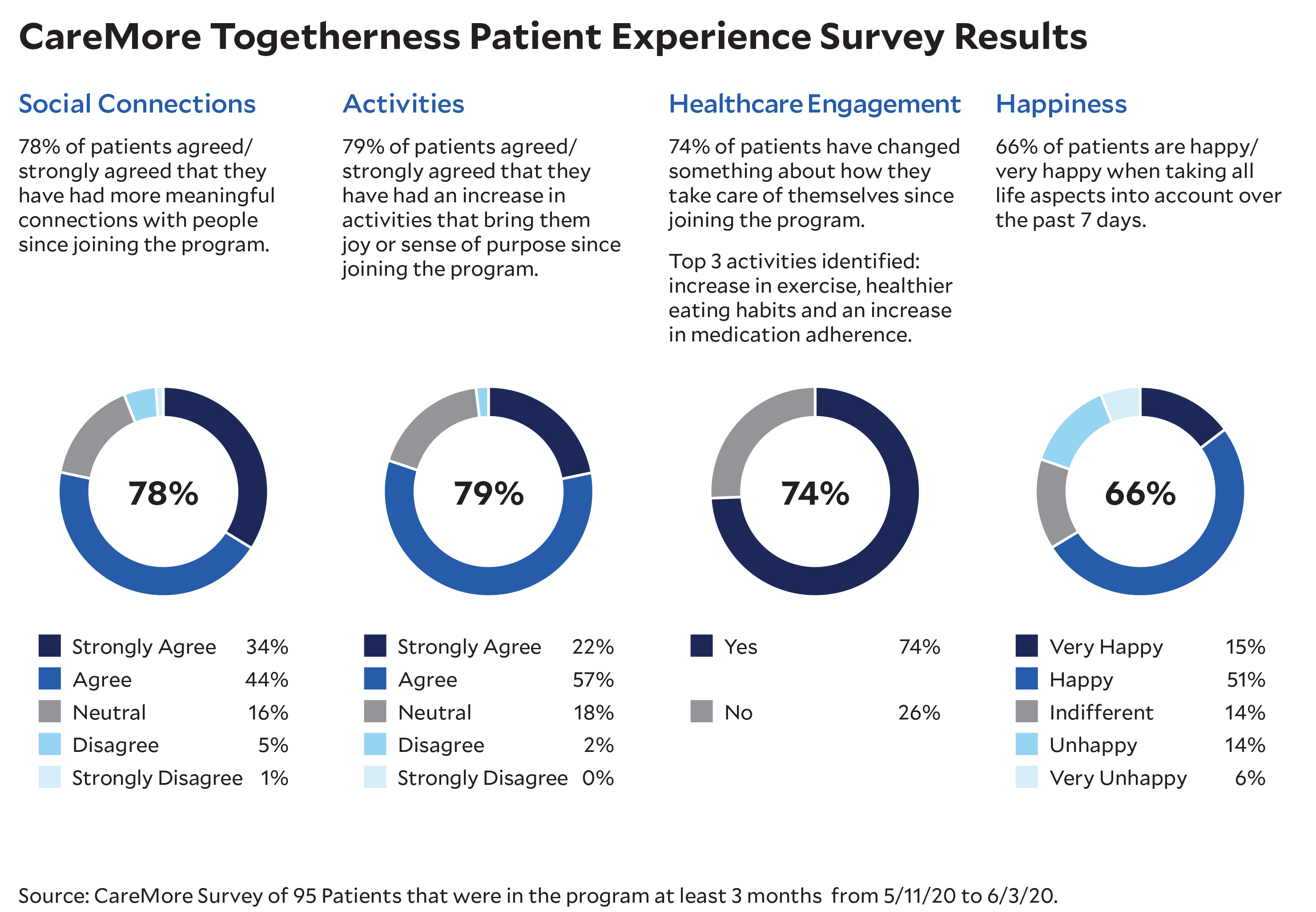
In addition, nearly a hundred Togetherness participants were recently polled about their experiences with the program. The data points show that participants are overwhelmingly happier, more active, more connected, and more committed to caring for their health as a result of their participation. (See graphic.) And their feedback was overwhelmingly positive according to those running the poll:
Patient feels like she is inspired to do more.
- Started to become motivated in taking care of self.
- Broadened social connections and learned to set personal goals and expectations.
- She has her confidence back.
- Wanting to go out more and speaking to her friends/ family more often.
- Anxiety isn’t so high and patient plans to start seeing a counselor.
Comments like these confirm that the program is changing lives.
Togetherness and COVID-19
Unfortunately, the COVID-19 pandemic has hindered CareMore and Aspire’s ability to implement another important part of the Togetherness program: graduation. The program generally lasts from nine to twenty-four months. At the end of that time, the idea has been that participants “graduate”—that they not only no longer experience persistent feelings of loneliness, but also that they can become mentors to others who are lonely. Regrettably, social distancing orders have delayed plans to expand the Togetherness initiative.
In the meantime, the Togetherness Program has become almost entirely telephonic—and more urgent than ever. Referrals into the program increased nearly nine-fold from February to March 2020. To meet the increased need, the health system has increased the number of Phone Pals by nearly 200 percent during the same timeframe. Nevertheless, physical distancing has made it impossible for many Togetherness program participants to maintain the in-person social connections they built over the past three years. In March, Sara expressed to Angelica for the first time in months that she felt “frightened,” and was concerned about regressing to her previously lonely state.
To ameliorate the effects of physical distancing, Phone Pals are trying different ways to safely keep people engaged, encouraging them to take walks in their neighborhoods and to participate in online classes through Nifty after Fifty, Silver Sneakers, and other such programs. Because most senior centers remain closed, the company mails out adult coloring books, puzzles and even checkers sets so members can play together while on the phone with their Phone Pals. Some members want to use FaceTime and Zoom to stay in touch with their families, so Phone Pals are teaching them to use these tools.
During COVID-19, the Togetherness Program has become almost entirely telephonic—and more urgent than ever.
Similarly, SCPs have begun to contact members via video-conferencing technologies. It is likely that many Phone Pals will do the same. One social group that had been meeting regularly in a neighborhood Care Center recently started meeting online to play games and participate in educational sessions on topics like coping with grief. Based on that group’s experience, the health system expects to expand the virtual groups to other neighborhoods.
Other Programs
The Togetherness program is likely the most comprehensive initiative of its kind. But it is by no means the only one. In the past several years, health providers and insurers, as well as private companies, have developed programs to address chronic loneliness and isolation. Many of these programs share similar traits. Some of them use the same resources. That’s not accidental. Just as many insurers work with the same providers, many of them are working with the same community resources and other services to treat loneliness. That’s especially true in the Medicare Advantage space, where health plans have increased flexibility to use their funding to address social drivers of health like loneliness.
Moreover, not all of the health systems are taking a “go-it-alone” approach to the problem. CareMore and Aspire, Humana and the University of Pittsburgh Medical Center Health Plan are all members of the Coalition to End Social Isolation & Loneliness, a national organization seeking to increase public awareness, promote research, and advocate for policy initiatives to combat the adverse consequences of social isolation and loneliness.
The health insurer Humana, rather than build a proprietary program to address loneliness among its members, instead worked with the Coalition to create Far From Alone, a campaign around health-related social needs that seeks to promote public health awareness and understanding of loneliness and social isolation, as well as provide resources for people to help them become less lonely.
One of Humana’s partners in the Far From Alone campaign is Papa, a private company whose reach spans several health systems. Papa provides virtual and in-person companionship, assistance, and transportation to older people. Its services are offered by health plans as a Medicare Advantage add-on at no cost to members. Humana, Aetna, and Priority Health all offer Papa services to their Medicare Advantage members.
“Papa Pals” fill a variety of needs, while providing companionship to lonely or socially isolated people. Pals help participants shop for groceries, take them to doctor appointments, and play games with them in their homes. One Papa Pal attended a wedding with a 90-year-old woman who was concerned that she might be a burden to her family on their special day.
Andrew Parker, Papa’s CEO, says “The core of our product is we provide companionship.” With that in mind, the company assesses clients for loneliness when they first sign up, using the Three Item UCLA Loneliness Scale. Parker says 50 percent of clients are identified as lonely before they begin using Papa, but more than 60 percent of those using the service feel less lonely (in other words, score lower on the scale) when they are re-evaluated after six months.
Michigan-based Priority Health offers Papa to its Medicare Advantage members. The insurer provides the service to members who are at high risk of hospitalization and have one or more chronic conditions that require intensive care coordination. Tami Hibbitts, Priority’s vice president of Senior Markets, said Priority partnered with Papa as part of a broader approach to addressing social drivers of health. “An important part of managing a chronic health condition is identifying and addressing underlying behavioral health and societal issues that may also be complicating the situation,” she said.
Hibbitts added that Priority views Papa as an especially important tool for treating older adults who live in remote, rural areas. With little access to transportation, they often cannot purchase fresh food or pick up prescriptions. Papa Pals can help these members improve their diets and increase their medication adherence.
About 500 Priority Health members have qualified for Papa’s services, and about 150 received a Papa visit prior to the COVID-19 outbreak. Since February, most visits have been virtual, though in some cases Papa Pals have gone out to peoples’ homes to help them sanitize high-touch surfaces like doorknobs and mailboxes.
Aetna
Aetna’s Resources for Living program connects Medicare Advantage members to a wide range of community services. Members access the program via a toll-free hotline which, since the onset of the COVID-19 epidemic, has been made available around the clock seven days a week.
A related initiative, Aetna Medicare Social Connectedness, is an outbound program that targets members deemed at risk for social isolation based on a proprietary algorithm that takes into account insurance claims and other member data. Members in this program may be connected with community services and referred for time-limited telephonic coaching. After such coaching is completed, members may also be referred to ongoing behavioral healthcare.
Aetna is gathering member experience metrics and other data around its Medicare Social Connectedness program, but recent data show that more than two-thirds of members reached engage in a full assessment, and nearly all engaged members are referred to one or more community resources. In the COVID-19 era, community resources like gyms and classes at senior centers are not appropriate, so the program has shifted its focus to connecting members with other relevant resources, such as food and medication delivery services and long-distance caregiving.
UnitedHealthcare
United Healthcare (UHC) assists its Medicare Advantage members who are socially isolated with referrals to and enrollment in government and social services. UHC reports that more than 290,000 members have indicated that they are socially isolated, and more than half of them have requested assistance with referrals to services. Those services include transportation and community programs that provide opportunities for social interaction.
In response to COVID-19, UHC has increased outreach to lonely and socially isolated members, checking on their well-being, connecting them to community resources and even directly shipping meals to members who have become food insecure. UHC’s nonprofit United Health Foundation also recently announced a $5 million collaboration with AARP Foundation to support older adults experiencing isolation and food insecurity during the COVID-19 crisis.
Commonwealth Care Alliance
In Massachusetts, Commonwealth Care Alliance (CCA) provides care to individuals who are dually eligible for Medicaid and Medicare. In July 2020 CCA began a new pilot program to address loneliness among its members. Somerville-Cambridge Elder Services (SCES), a social services provider that currently supports about 1,000 CCA members, will screen 100 members for loneliness using the three-question UCLA Loneliness Scale. Larry Gottlieb, CCA’s chief quality officer, said he expects as many as 30 percent to 50 percent of screened members to test positive for loneliness, and perhaps even more, given COVID-19 social distancing recommendations.
Those members deemed at high-risk for loneliness will be offered support though community-based programs and behavioral health consultations as appropriate. People who are deemed at medium-risk will be referred to “Phone Buddies”—CCA employees who volunteer to call their buddies at least once a week for fifteen minutes. Phone Buddies will receive relevant training and support from behavioral health co
‘ “Quite simply, human relationship is as essential to our well-being as food and water,” wrote former Surgeon General Vivek Murthy.’
CCA is undertaking the programs because “Loneliness and social isolation are prevalent among [older adults] and even more prevalent among [older adults] with fewer resources,” says Gottlieb. “Resolving that can make a difference in quality of life and clinical outcomes.”
CCA plans to evaluate the program in early fall. If the organization finds that rates of loneliness decrease and that participants show signs of engagement, it will expand the program to other members.
Conclusion
“Quite simply, human relationship is as essential to our well-being as food and water,” wrote former Surgeon General Vivek Murthy (Murthy, 2020). While drafting this article, the authors find themselves wrapped up in layers of irony. The great pandemic of our era, COVID-19, has become the single most discussed topic among anyone with even a fleeting connection to the healthcare industry. At the same time, another massive epidemic, of loneliness, often goes unaddressed.
The COVID-19 pandemic is exacerbating the loneliness epidemic and has thrust the issue to the forefront. There is a responsibility within the healthcare sector to normalize conversations about loneliness, among other medical and social issues, within care planning and delivery. Loneliness and isolation should be assessed and treated in the same way as other issues concerning health—through screening and appropriate intervention. More important, as the healthcare sector takes the lead to prevent and reverse the adverse effects of loneliness and isolation, it must do it together as a community through meaningful connections and partnerships.
Robin Caruso, LCSW, is chief togetherness officer, Shaden Marzouk, MD, MBA, is president, and Serena Foong is staff vice president, Strategic Initiatives; all with CareMore and Aspire Health, based in Los Angeles, California. Vivek Garg, MD, MBA, is former chief medical officer of CareMore and Aspire Health.
References
Hamar, B., et al. 2013. “Impact of a Senior Fitness Program on Measures of Physical and Emotional Health and Functioning.” Population Health Management 16(6): 364-72. doi: 10.1089/pop.2012.0111.
Holt-Lunstad J., Smith T. B., and Layton J. B., 2010. “Social Relationships and Mortality Risk: A Meta-analytic Review.” PLOS Medicine 7(7). doi.org/10.1371/journal.pmed.1000316.
Murthy, V. H. 2020. Together: The Healing Power of Human Connection in a Sometimes Lonely World. New York: HarperCollins.
National Institute on Aging. 2019. “Social Isolation, Loneliness in Older People Pose Health Risks.” Retrieved Jun 17, 2020.
Perissinotto, C., Cenzer, I. S., Covinsky, K. E. 2012. “Loneliness in Older Persons: A Predictor of Functional Decline and Death.” Archives of Internal Medicine 172(14): 1078-84.
Williams, V. 2019. “How Aerobic Exercise Benefits the Brain—Especially As You Age.” U.S. News & World Report. Retrieved June 17, 2020.











